
Lancet Review
Comparative efficacy and acceptability of 12 new-generation
antidepressants: a multiple-treatments meta-analysis
Dr Andrea Cipriani et al
The Lancet, Volume 373, Issue 9665, Pages 746 - 758, 28 February 2009. Full
text pdf
Summary
Background
Conventional meta-analyses have shown inconsistent results for efficacy of second-generation
antidepressants. We therefore did a multiple-treatments meta-analysis, which
accounts for both direct and indirect comparisons, to assess the effects of
12 new-generation antidepressants on major depression.
Methods
We systematically reviewed 117 randomised controlled trials (25 928 participants)
from 1991 up to Nov 30, 2007, which compared any of the following antidepressants
at therapeutic dose range for the acute treatment of unipolar major depression
in adults: bupropion, citalopram, duloxetine, escitalopram, fluoxetine, fluvoxamine,
milnacipran, mirtazapine, paroxetine, reboxetine, sertraline, and venlafaxine.
The main outcomes were the proportion of patients who responded to or dropped
out of the allocated treatment. Analysis was done on an intention-to-treat basis.
Findings
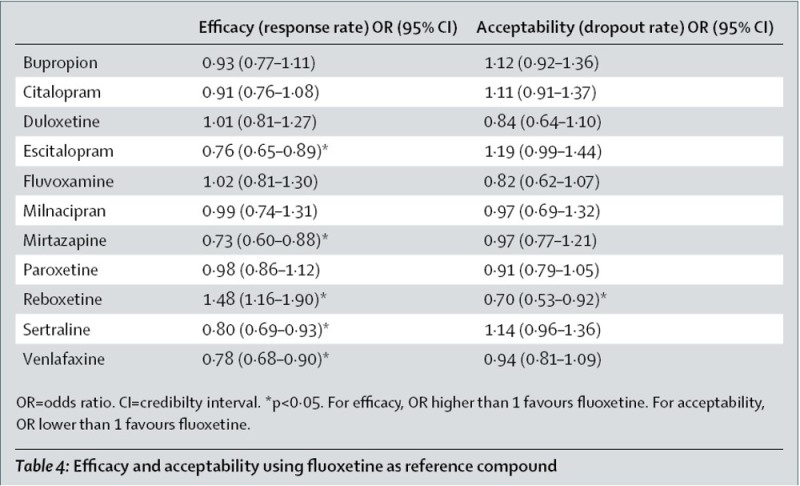
Mirtazapine, escitalopram, venlafaxine, and sertraline were significantly more
efficacious than duloxetine (odds ratios [OR] 1·39, 1·33, 1·30
and 1·27, respectively), fluoxetine (1·37, 1·32, 1·28,
and 1·25, respectively), fluvoxamine (1·41, 1·35, 1·30,
and 1·27, respectively), paroxetine (1·35, 1·30, 1·27,
and 1·22, respectively), and reboxetine (2·03, 1·95, 1·89,
and 1·85, respectively). Reboxetine was significantly less efficacious
than all the other antidepressants tested. Escitalopram and sertraline showed
the best profile of acceptability, leading to significantly fewer discontinuations
than did duloxetine, fluvoxamine, paroxetine, reboxetine, and venlafaxine.
Interpretation
Clinically important differences exist between commonly prescribed antidepressants
for both efficacy and acceptability in favour of escitalopram and sertraline.
Sertraline might be the best choice when starting treatment for moderate to
severe major depression in adults because it has the most favourable balance
between benefits, acceptability, and acquisition cost.
It expressed judgments about the relative efficacy and acceptability of different drugs, more clearly than the ACP papers.
Efficacy The cumulative probabilities of being among the four most effective treatments were:
|
Acceptability The cumulative probabilities of being among the four most acceptable treatments were:
|
Efficacy |
Acceptibility Higher is better |

Ranking for efficacy (solid line) and acceptability (dotted line).
Lines over on the left are better.
Ranking indicates the probability to be the best treatment, the second best,
the third best, and so on, among the 12 antidepressants.
This makes the winners (escitalopram, sertraline, mirtazapine, and venlafaxine) obvious, but also illustrates how badly reboxetine and fluvoxamine do. I was surprised at the apparent difference between venlafaxine and duloxetine, which have seemed very similar to me, with, if anything, duloxetine having the advantage.